Free Advance Beneficiary Notice of Non-coverage Template
Free Advance Beneficiary Notice of Non-coverage Template
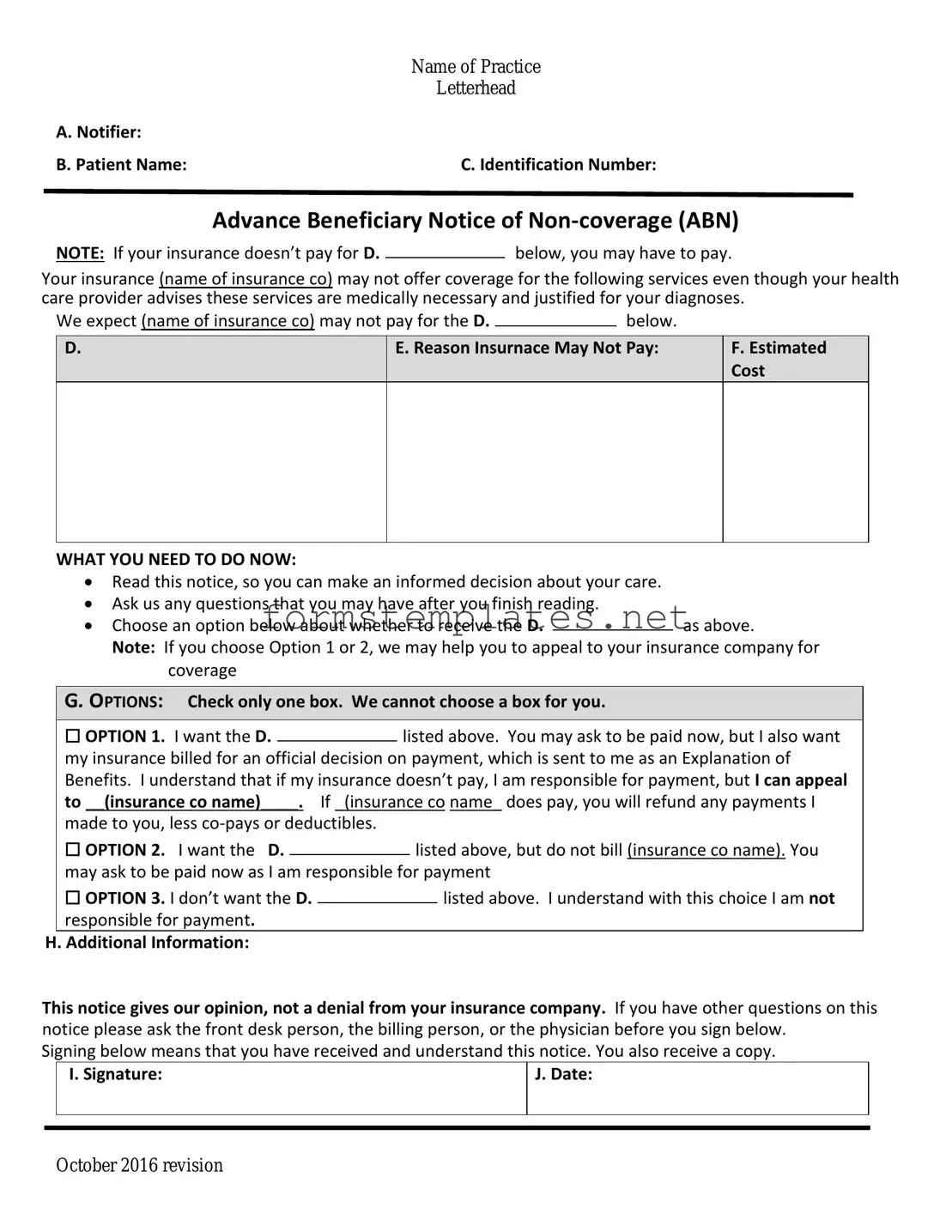
The Advance Beneficiary Notice of Non-coverage (ABN) form plays a crucial role in the Medicare system, serving as a communication tool between healthcare providers and beneficiaries. When a provider believes that a service may not be covered by Medicare, they issue this form to inform patients about the potential financial implications. The ABN outlines the specific service in question, explains why it may not be covered, and provides beneficiaries with options to either proceed with the service or decline it. This form is essential for ensuring that patients are aware of their financial responsibilities before receiving care. By signing the ABN, beneficiaries acknowledge that they understand the potential for non-coverage and agree to pay for the service if Medicare denies the claim. It is vital for patients to carefully review the information presented on the ABN, as it can significantly impact their out-of-pocket costs and overall healthcare decisions. Understanding the nuances of the ABN can empower beneficiaries to make informed choices regarding their medical care and financial obligations.
The Advance Beneficiary Notice of Non-coverage (ABN) form is an important document in the Medicare system. Here are some key takeaways to understand its purpose and use:
When filling out the Advance Beneficiary Notice of Non-coverage (ABN) form, it's important to be careful and thorough. Here’s a list of six things you should and shouldn't do:
The Advance Beneficiary Notice of Non-coverage (ABN) is an important document that informs patients when Medicare may not cover a service or item. Alongside the ABN, several other forms and documents are commonly used in healthcare settings to ensure that patients understand their rights and responsibilities. Below is a list of these documents, each serving a unique purpose.
Understanding these documents is crucial for patients navigating their healthcare options. Each form plays a role in protecting patient rights and ensuring transparency in the billing and coverage process.
Ca Reg 262 - The acquisition number is specifically for dismantlers and must be completed if applicable.
Printable Five Wishes Document Pdf - Using this document means your healthcare preferences are well-documented and legally valid.
When considering legal protection for your information, it’s important to understand the implications of a trusted Non-disclosure Agreement resource. This form can be vital for maintaining confidentiality in your business dealings.
Dekalb County Water Application Online - Water service requests must be submitted through this official form.
The Advance Beneficiary Notice of Non-coverage, commonly referred to as the ABN, is a form that healthcare providers use to inform patients that Medicare may not cover a specific service or item. This notice is important because it allows patients to understand their financial responsibilities before receiving care. By signing the ABN, patients acknowledge that they may have to pay for the service if Medicare denies coverage.
A healthcare provider should issue an ABN when they believe that Medicare may not pay for a service or item. This can occur in various situations, such as:
Providers must issue the ABN before the service is rendered, allowing patients to make informed decisions about their care and potential costs.
If a patient chooses not to sign the ABN, they may still receive the service. However, this decision carries risks. If Medicare denies coverage for the service, the patient will be responsible for the full cost without any prior acknowledgment of potential out-of-pocket expenses. It is crucial for patients to understand their options and the implications of not signing the form.
It is advisable to seek assistance from a Medicare representative or a healthcare advocate when navigating the appeals process.
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision
| Fact Name | Description |
|---|---|
| Purpose | The Advance Beneficiary Notice of Non-coverage (ABN) informs patients that Medicare may not cover a specific service or item. |
| When to Use | Providers must issue the ABN when they believe Medicare will deny payment for a service or item. |
| Patient Rights | Patients can choose whether to receive the service after being informed of potential non-coverage. |
| Signature Requirement | Patients must sign the ABN to acknowledge their understanding of the potential for non-coverage. |
| State-Specific Forms | Some states may have additional requirements or specific forms governed by local laws. |
| Documentation | Providers must keep a copy of the signed ABN in the patient's medical record for compliance purposes. |
| Impact on Billing | If a patient receives a service after signing the ABN, they may be billed directly if Medicare denies coverage. |
After receiving the Advance Beneficiary Notice of Non-coverage (ABN), it’s important to fill it out correctly. This form helps you understand your financial responsibility for certain services. Follow these steps to complete the form accurately.
Once you have completed the form, keep a copy for your records. Submit the original to your healthcare provider. They will use this information to determine your financial obligations for the services listed.