Free Annual Physical Examination Template
Free Annual Physical Examination Template
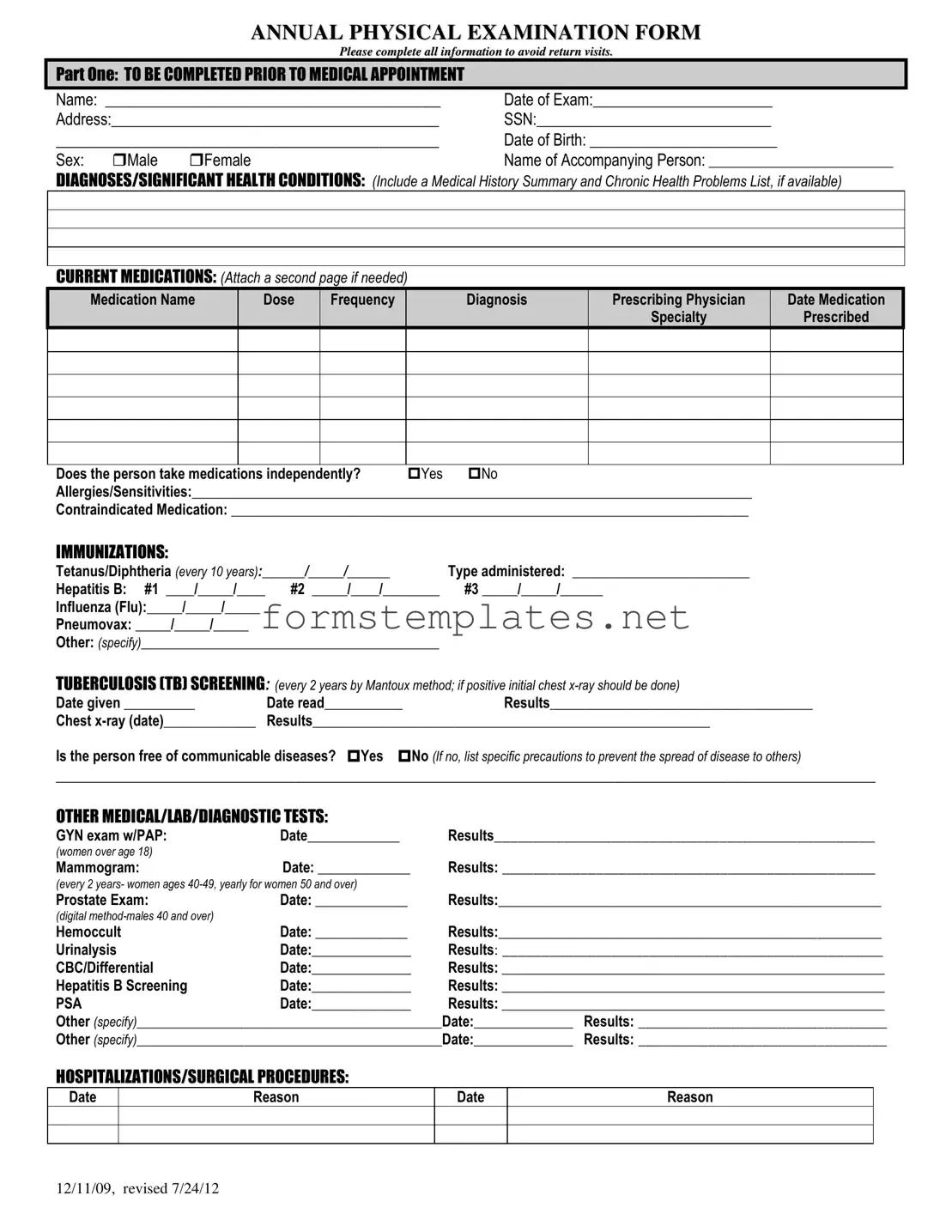
The Annual Physical Examination form plays a crucial role in ensuring that individuals receive comprehensive healthcare. It is designed to gather essential information before a medical appointment, streamlining the process for both patients and healthcare providers. The first section of the form requires personal details such as name, date of birth, and address, along with a summary of medical history and current medications. It also prompts for information on allergies, immunizations, and any significant health conditions. Following this, the form includes a thorough evaluation of various health systems, assessing everything from blood pressure to vision and hearing. Additional sections cover past hospitalizations and surgeries, along with recommendations for health maintenance and any necessary follow-ups. Completing this form accurately helps avoid return visits and ensures that healthcare providers have a clear understanding of the patient's health status. By taking the time to fill it out, patients contribute to a more efficient and effective healthcare experience.
1. Complete All Sections: Fill out every part of the Annual Physical Examination form before your medical appointment. Missing information may lead to delays and require additional visits.
2. Provide Accurate Medical History: Include a summary of your medical history and any chronic health problems. This information is crucial for your healthcare provider to understand your health status.
3. List Current Medications: Document all medications you are currently taking. This includes the name, dosage, frequency, and prescribing physician. Attach an additional page if necessary.
4. Update Immunization Records: Record your immunizations accurately. Ensure that dates and types of vaccinations are clearly noted, especially for Tetanus, Hepatitis B, and Influenza.
5. Note Any Allergies: Clearly state any allergies or sensitivities you have. This information is vital for preventing adverse reactions during treatment.
6. Review and Sign: After completing the form, review all entries for accuracy. Sign and date the form to confirm that the information provided is correct and complete.
When filling out the Annual Physical Examination form, it's essential to approach the task with care. Here are some helpful tips on what to do and what to avoid:
When preparing for an annual physical examination, several important documents and forms may be required in addition to the Annual Physical Examination form. Each of these documents plays a vital role in ensuring a comprehensive assessment of an individual's health. Below is a list of commonly used forms that accompany the annual physical examination.
Having these documents ready can streamline the examination process and ensure that healthcare providers have all the necessary information to deliver effective care. It is advisable to complete and bring these forms to your appointment to avoid any delays or additional visits.
How to Make a Family Crest - A historical representation of community and pride.
Obtaining the Aaa International Driving Permit Application form is essential for anyone planning to drive abroad, as it grants the legal right to operate vehicles in participating countries. This can greatly enhance your travel experience, allowing for greater exploration and adventure. For more information or to begin the application process, visit pdftemplates.info.
Cancel Melaleuca - The customer service number is a helpful resource for your needs.
The Annual Physical Examination form is designed to gather essential health information before your medical appointment. It helps your healthcare provider understand your medical history, current medications, and any significant health conditions you may have.
In Part One, you must fill in your personal details, including your name, date of birth, and address. You will also need to list any significant health conditions, current medications, allergies, and immunization history. This section ensures that your provider has a comprehensive view of your health status.
List each medication by name, along with the dose, frequency, diagnosis, prescribing physician, and the date prescribed. If you take multiple medications, attach an additional page if necessary. Indicate whether you take medications independently.
You should provide information on your immunizations, including:
Be sure to include the dates administered and the type of vaccine given.
If you have a communicable disease, you must indicate this on the form. Additionally, you should list specific precautions to prevent spreading the disease to others. This information is crucial for the safety of both you and the healthcare staff.
In this section, report any relevant medical tests you have undergone. This includes:
Include the date of the test and the results.
If there has been any change in your health status, you must indicate this on the form. Provide details about the changes, as this information is vital for your healthcare provider to offer appropriate care.
Recommendations for health maintenance may include advice on lab work, treatments, therapies, exercise, hygiene, and weight control. Your healthcare provider will use this information to help you maintain or improve your health.
Inaccurate or incomplete forms may result in return visits or delays in your care. It is essential to provide accurate information to ensure that your healthcare provider can give you the best possible care.
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
| Fact Name | Details |
|---|---|
| Purpose | The Annual Physical Examination form is designed to collect comprehensive health information before a medical appointment. |
| Required Information | Patients must provide personal details, including name, date of birth, address, and social security number. |
| Medical History | It includes sections for current medications, allergies, and significant health conditions, ensuring a thorough review of the patient's medical background. |
| Immunization Records | The form requires documentation of immunizations, including tetanus, hepatitis B, and flu shots, which are essential for preventive care. |
| Screening Tests | Patients must report results from various screenings, such as TB tests, mammograms, and prostate exams, depending on age and gender. |
| Physical Examination | It includes a section for vital signs and a general physical examination to assess overall health status. |
| Recommendations | The form allows healthcare providers to make personalized health maintenance recommendations based on the examination findings. |
| State-Specific Laws | In some states, specific laws may govern the use of such forms, including requirements for patient consent and data privacy. |
Completing the Annual Physical Examination form is an important step in ensuring that your health needs are met. By providing accurate and thorough information, you help your healthcare provider deliver the best possible care. The following steps will guide you through filling out the form effectively.
Once you have completed the form, review it carefully to ensure all information is accurate and complete. This will help avoid any delays during your medical appointment. Bring the form with you to your appointment for a smooth and efficient visit.